 [1]Here we go. I believe the common treatment protocol for piriformis syndrome is not addressing the real issue. I understand this may stir some clinical debate, but as a PT who treats the cause of pain and not the area of pain, it doesn’t make sense to just treat the piriformis muscle. Currently, stretching, manual therapy and ultrasound (hello 1975!) are the main-stays of treating this syndrome. But, clinically, I have consistently found a different reason for piriformis syndrome.
[1]Here we go. I believe the common treatment protocol for piriformis syndrome is not addressing the real issue. I understand this may stir some clinical debate, but as a PT who treats the cause of pain and not the area of pain, it doesn’t make sense to just treat the piriformis muscle. Currently, stretching, manual therapy and ultrasound (hello 1975!) are the main-stays of treating this syndrome. But, clinically, I have consistently found a different reason for piriformis syndrome.
Before we go any further, if you have symptoms of sciatica it is important to have a differential diagnosis. Ensure your medical professional (MD, DO, PT, etc.) is clearing the spine first.
 [2]What is Piriformis Syndrome?
[2]What is Piriformis Syndrome?
Compression of the sciatic nerve by the piriformis muscle, causing pain into the buttock and leg.
Piriformis syndrome was first described in a publication by Daniel Robinson, MD in 1947. It was an important article, giving an alternative explanation to sciatic pain. However, a pivotal piece of that article seems to have lost its way…
Common Symptoms of Piriformis Syndrome
- buttock pain that may or may not travel down the leg
- pain that is aggravated by sitting
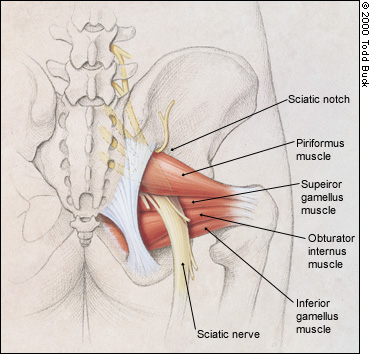
- pain at the sciatic notch: a landmark where the nerve runs
Popular Treatments for Piriformis Syndrome
- Releasing the piriformis muscle via manual therapy or massage. This usually entails digging an elbow or fist into the painful muscle. Read below for further explanation.
- Stretching the piriformis. What if the muscle is long and taut and not short and thick? In general, it is usually not a length issue.
- Ultrasound. Honestly, I’ve used ultrasound maybe 10 times in my entire career. I’m in my 9th year of clinical care. You can see how important I think it is.
- Botulinum toxin injections to relax the hypertrophic piriformis muscle. Research is inconclusive about the long term effects.
- Surgery. Yes, actually cutting the muscle to take pressure off the nerve. This seems a little drastic, especially if not necessary.
As stated above, one of the common treatments for this syndrome is to excessively dig into the painful muscle, trying to release any trigger points. Sometimes there are trigger points, but what I most often hear from patients is that someone is releasing pain over the sciatic nerve! It sends chills up my spine. Because the sciatic nerve runs under the piriformis, applying pressure to this area elicits intense buttock and leg pain. But then something magical happens. The pain fades away and the patient feels relief. It is not because the muscle is being released but because the pressure begins to cut of the neurovascular supply to the sciatic nerve. This is the same idea as sitting on a tennis ball (which always makes me cringe!) to “release” the muscle. Shutting off blood flow to the sciatic nerve is not the treatment answer. Figuring out WHY the piriformis is compressing the sciatic nerve is the KEY to treating this syndrome. Once again, I find the Gluteus Maximus (GMax) and Gluteus Medius (GMed) are just plain lazy.
Causes of Piriformis Syndrome
- Abnormal emergence of the sciatic nerve. Sometimes it will pierce through the piriformis muscle making it more vulnerable to compression. Research states this occurs ~20% of the time.
- Fibrosis or adhesions of the piriformis muscle from trauma.
- Myositis ossificans of the muscle from blunt trauma. Calcification of the muscle occurs. This is rare.
- Hypertrophy of the Piriformis Muscle. This is the most common reason. But, here’s the clinical question: why is there muscle hypertrophy?
Ok, let’s dive into some specifics to better understand why I don’t treat the piriformis when someone presents with piriformis syndrome.
What is the Piriformis Muscle?
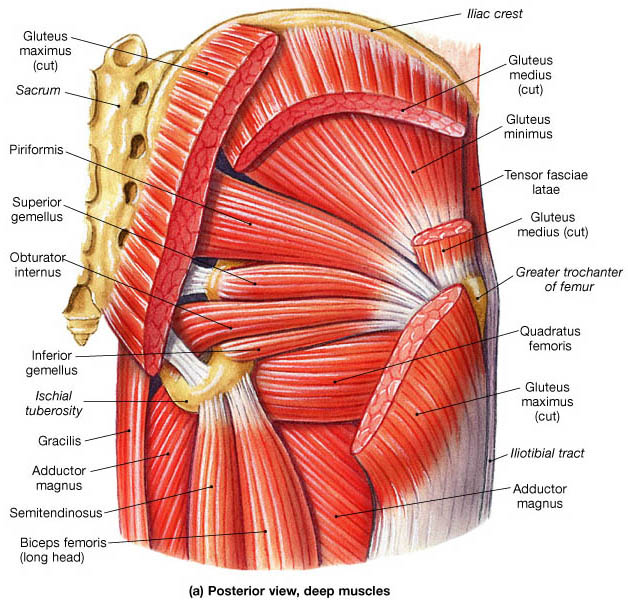
 [3]Piriformis. It’s kind of of fun word to say. It is derived from the latin words pirum and forma. Pirum means pear, forma means shape. So, it is a long, triangular muscle that kinda sorta resembles a pear… a flat, squishy pear. It is an interesting muscle in that it can assist with hip internal rotation when the hip is flexed (in front of you) and with external rotation when the hip is extended (behind you). It will also assist with abduction (raising the leg to the side). It is a muscle that protects the sciatic nerve as it starts to travel down the leg, acting like a sling from the sacrum to the greater trochanter on the femur. Notice that the piriformis is an assistant…to all of the motions. And, clinically, I see it try to take on an entirely new motion: extension. This sets the muscle up to be bulky, hypertrophic and dysfunctional.
[3]Piriformis. It’s kind of of fun word to say. It is derived from the latin words pirum and forma. Pirum means pear, forma means shape. So, it is a long, triangular muscle that kinda sorta resembles a pear… a flat, squishy pear. It is an interesting muscle in that it can assist with hip internal rotation when the hip is flexed (in front of you) and with external rotation when the hip is extended (behind you). It will also assist with abduction (raising the leg to the side). It is a muscle that protects the sciatic nerve as it starts to travel down the leg, acting like a sling from the sacrum to the greater trochanter on the femur. Notice that the piriformis is an assistant…to all of the motions. And, clinically, I see it try to take on an entirely new motion: extension. This sets the muscle up to be bulky, hypertrophic and dysfunctional.
What is the Sciatic Nerve?
The sciatic nerve is a large nerve that travels down the back of the leg to innervate the hamstrings, part of the adductor magnus, the lower leg and foot muscles. It is a thick cord of nerve fibers, receiving input from L4, L5, S1, S2, and S3. (Now you can see the importance of clearing the spine first!) The nerve travels to the back of the leg behind the piriformis muscle and courses down the center of the thigh. Around the knee, it breaks into 2 branches: the tibial nerve and common peroneal nerve. It is a long, important nerve that, when irritated, causes pain in the buttock and leg.
What is Muscle Hypertrophy?
 [4]Hypertrophy of muscle occurs as an adaption to heavy load or use. It is an increase in the size of the muscle fibers and cellular components; the cross-sectional thickness actually increases. Hypertrophy is a sign that the muscle is receiving A LOT of neural input to make the muscle contract. Can you imagine if your piriformis had muscle hypertrophy and to decrease it, someone said: “Just stretch.”
[4]Hypertrophy of muscle occurs as an adaption to heavy load or use. It is an increase in the size of the muscle fibers and cellular components; the cross-sectional thickness actually increases. Hypertrophy is a sign that the muscle is receiving A LOT of neural input to make the muscle contract. Can you imagine if your piriformis had muscle hypertrophy and to decrease it, someone said: “Just stretch.”
Back to the question: Why is there hypertrophy of the piriformis muscle? Mr. and Mrs. GMax and GMed have decided to not pull their weight! This is not the fault of the piriformis. Our bodies are incredibly smart and will compensate however needed. If GMax is not doing its job in all three planes (extension, abduction and external rotation), the piriformis says: “Ooh, pick me! I will help you!” If the GMed (main abductor) is lazy, the piriformis, once again, begins to work harder. So, can you see that simply releasing the piriformis, stretching the piriformis and moving ultrasound gel over the piriformis will not fix the real problem? Teaching our glutes how to work is the answer! In addition, making sure the main rotators of the hip (gemellis, obdurators, quadratus femoris) are doing their job too.
Above I mentioned that Dr. Robinson originally described piriformis syndrome in 1947. And, in his paper he also found that gluteal atrophy was more likely and a cardinal criteria of piriformis syndrome. Let me re-phrase that. Atrophy of the glutes is associated with piriformis syndrome. Hmmm…
If the piriformis is the only area getting treatment, the syndrome will never truly resolve. It is imperative to teach the glutes and hip rotators how to work in order to decrease the load on the piriformis.
Increased work load on the glutes = decreased work load on the piriformis
Decreased work load on the piriformis = decreased hypertrophy
Decreased hypertrophy = decreased compression on the sciatic nerve
Decreased compression on the sciatic nerve = pain resolution!
I hope this makes sense now.
A Research Case Study
 [5]A 28 y.o. competitive cyclist had an MRI showing hypertrophy of the left piriformis. He was given a prescription of massage, stretching and botulinum toxin injections. This combination did not work, so the cyclist had 2/3rds of the piriformis cut
[5]A 28 y.o. competitive cyclist had an MRI showing hypertrophy of the left piriformis. He was given a prescription of massage, stretching and botulinum toxin injections. This combination did not work, so the cyclist had 2/3rds of the piriformis cut
What muscles do I consistently educate about in my blogs, especially when it applies to cyclists and runners? The weakness of the glutes…something to ponder.
© 2015 and Beyond! ALL BLOG CONTENT at duncansportspt.com by Lori Duncan PT
BLOG TALK PODCAST:
Blog Talk – Piriformis Syndrome [6]
ABOUT THE AUTHOR
 Lori Duncan, DPT, MTC, CPT is a respected Physical Therapist, Manual Therapist and Pilates instructor in Lafayette, CO. Lori is passionate about preventive physical therapy and education and is a nationally recognized presenter. She can be reached at [email protected]. You can also follow Duncan Sports Therapy + Wellness on Facebook [7] & Instagram [8] for more free tips and information.
Lori Duncan, DPT, MTC, CPT is a respected Physical Therapist, Manual Therapist and Pilates instructor in Lafayette, CO. Lori is passionate about preventive physical therapy and education and is a nationally recognized presenter. She can be reached at [email protected]. You can also follow Duncan Sports Therapy + Wellness on Facebook [7] & Instagram [8] for more free tips and information.
References
Fouasson-Chaillou A, Dubois C, Dauty M. Piriformis syndrome diagnosis: on two professional cyclists. Ann Phys Rehab Med. 57(4):2014;268-274.
Papadopoulos EC, Khan SN. Piriformis syndrome and low back pain: a new classification and review of the literature. Orthop Clin N Am. 35:2004;65-71.