Hip labral tear. Hip labral impingement. These are quite the “buzz words” in orthopedic medicine. Technically called FAI (Femoral Acetabular Impingement), these are diagnosed quite frequently. Research states between 22-55% of the population is walking around with a labral hip tear. But, here’s the question: are people actually getting more hip labral tears these days? Maybe. Maybe not. A more likely explanation: we finally have imaging to prove that a hip labral tear exists. Ok, fine. But, just because we have imaging that can finally diagnose a labral tear, does it really require surgery? These arthroscopic surgeries are very popular (yes, I just used the word “popular” for a surgery). Most athletes, elite and recreational, think this is the golden ticket to recovery. But it’s not necessarily true. FAI surgeries are far from perfect. I always tell my patients: “There is a time and place for surgery. When you need it, go get it.” But, surgery should be the last resort, not the first. So, if you think you MAY have a hip labral tear, consider the first recommendation of research: give physical therapy a good go!
This blog is inspired by several patients over the past few years. Some weren’t sure (and they did have a labral tear), some were sure (and they didn’t have a labral tear). But, all of them were motivated to heal their hip pain without surgery. Remember, PT is not harmful. And, with a correct diagnosis, most (not all) people can heal without surgical intervention.
Ok. Let’s all get on the same page. What are we talking about?
Anatomy Review: The Hip and its Labrum
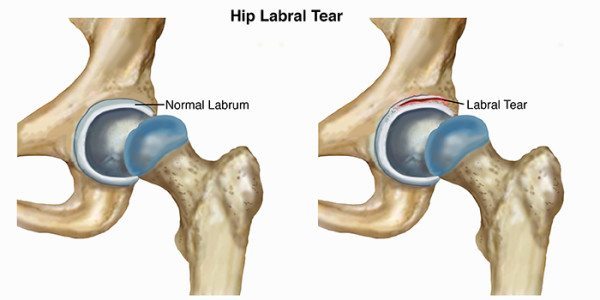
(picture from APTA [1] website)
The hip consists of the pelvic bone and femur. The head of the femur (the blue part above) glides around the acetabulum (hole in the pelvis) to create movement.
The hip labrum is an intrinsic (internal) source of hip stability. The labrum acts as a suction around the hip joint to provide extra stability, along with the ligaments and muscles. In addition, it creates extra coverage and lubrication to the hip joint. Basically, the labrum helps keep the hip happy and healthy.
What is a Femoral Acetabular Impingement (FAI)?
There are three main types: pincer, cam and combo
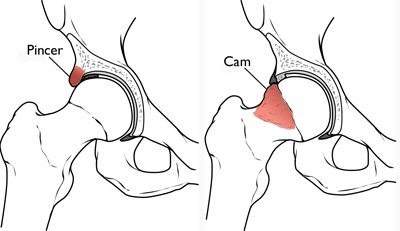
(image from http://orthoinfo.aaos.org/)
Pincer- Bone on the acetabulum extends over the natural rim and impinges the femoral head. Basically, blame it on the pelvis.
Cam- The femoral head is not round enough to glide smoothly in the hip socket and can bother the labrum. Blame this on the femur.
Combo- Cam + Pincer issues.
Possible Signs of FAI
- Anterior (front) hip and groin pain
- Lateral (side) hip or leg pain
- Anterior thigh pain
- Glute pain
- Clicking or sensation of “pop” during certain movements
- Decreased range of motion and hip tightness
- Pain with hip flexion, squats
When you look at these symptoms above, almost everyone reading will start to wonder if they have a hip impingement, right? I know you’re thinking: “Well, yes, I do have glute pain and some thigh pain. And, you know, now and then my hip does pop.” That’s why it is IMPERATIVE you have a medical professional test your symptoms and not rely on Mr. Google for a diagnosis.
Medicine continues to point in the direction of physical therapy as a first line of intervention for orthopedic issues. It’s more cost effective and an experienced PT will know if you need a referral to an orthopedic surgeon. So what does the research say about FAI? Try a course of non-operative intervention (“aka physical therapy”) for at least 10 to 12 weeks. The physical therapist will be able to clinically diagnose a possible FAI. Here are some common tests I use for a diagnosis:
- Scour test
- FABER
- Hip impingement test
- Hip internal rotation ROM
Note: I have withheld information on what these tests entail because only a medical professional should be performing and diagnosing the outcomes of these tests. There can be A TON of misinterpretation if they are not conducted correctly.
If any or all of these tests are positive, the patient may have a possible labral tear. Does that mean I send them for a MRI? Maybe, maybe not. Some people feel better having a picture of their possible tear. Most people would rather not spend the money if they are going to try PT first. And, a visit to an orthopedic surgeon (with or without a MRI) will go something like this: “Go try physical therapy for a few months. If it’s not better, then come back.”
One of the most consistent findings of hip labral tears is myofascial (muscle and fascia) pain of the quads, hip, back and glutes. Manual therapy and specific physical therapy exercises can be the magic ticket to reducing this pain. And, then, their hip impingement symptoms are minimal to none. So, wouldn’t it be nice to know if your hip pain is really from the impingement or just a myofascial syndrome? I sure hope you’re nodding your head “yes.”
If your hip symptoms don’t improve in 12 weeks, then start the expensive MRI, surgical consult route. At least by then you will be informed and a little stronger going into surgery.
Clinical Case Studies
17 year-old track and field player
 While hurdling, he felt a pop and then sudden pain in his right hip. Although his symptoms improved slightly with strength training, his parents decided to have an MRI. The MRI showed a possible labral tear, but nothing conclusive. Significant findings at the initial evaluation:
While hurdling, he felt a pop and then sudden pain in his right hip. Although his symptoms improved slightly with strength training, his parents decided to have an MRI. The MRI showed a possible labral tear, but nothing conclusive. Significant findings at the initial evaluation:
- Right hip pain, deep ache (1/10) to sharp pain (8/10)
- Pain with hurdling and hip flexion
- Positive scour test and FABER test (minimal)
- Internal rotation was within normal limits
- Weak glutes and intrinsic core
After 3 visits in 4 weeks, the patient reported 70% improvement of symptoms. His physical therapy program consisted of a Pilates program, a non-weight bearing to weight-bearing strength program and specific stretching. At 4 weeks, he was back to hurdling 2x/week with right hip tightness (no pain) that he could easily relieve with his PT exercises. He was diligent about doing his Pilates program and strength program 2-3x/week. Each program was 10-12 minutes in length (that’s it!). Note: I treated this patient remotely. He never received one manual treatment. He healed himself by doing the right exercises to stabilize and strengthen his hip.
44 year old competitive cyclist and avid mountain climber
 This patient came to see me three months after his initial symptoms. He stated left hip tightness during his cycle season, but in October of that year he had significant left hip pain while working out with his personal trainer. Significant findings at the initial evaluation:
This patient came to see me three months after his initial symptoms. He stated left hip tightness during his cycle season, but in October of that year he had significant left hip pain while working out with his personal trainer. Significant findings at the initial evaluation:
- Left hip tightness that radiated to his anterior leg
- Tenderness of the anterior hip muscles (rectus femoris, tensor fascia lata) and glute medius
- Positive scour and FABER test
- Hip internal rotation limited by pain and “slide” sensation
- Weak glutes and intrinsic core
After 3 months of physical therapy, the patient reported significant improvement of his symptoms. He continued with PT every other week, then once a month. At 8 months, this patient was back to cycling, personal training and climbing with minimal left hip tightness, no pain. His physical therapy program consisted of: manual therapy, Pilates-based therapeutic exercise, stretching and non weight-bearing to weight-bearing strength and stability. He worked his tail off, avoided surgery and returned to ALL of his activities.
Take Home Point
- If you think you have a hip labral tear, try physical therapy first for at least 10-12 weeks. Ensure your hip is surgery worthy!
© 2016 & Beyond. ALL BLOG CONTENT at duncansportspt.com by Lori Duncan PT
BLOG TALK PODCAST:
Blog Talk – Hip Labral Tear [2]

ABOUT THE AUTHOR
Lori Duncan, DPT, MTC, CPT is a respected Physical Therapist, Manual Therapist and Pilates instructor in Lafayette, CO. Lori is passionate about preventive physical therapy and education and is a nationally recognized presenter. She can be reached at [email protected]. You can also follow Duncan Sports Therapy + Wellness on Facebook [3] & Instagram [4] for more free tips and information.
Research
Phillippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction. J Bone Joint. 2009;91:16-23.
Cashman GE, Mortenson WB, Gilbart MK. Myofascial treatment for patients with acetabular labral tears: a single-subject research design study. J Orthop Sports Phys Ther. 2014;44:604-14.