When was the last time you thought: “I think I’ll go to the gym and work on my rotator cuff.” We should think this way, but we don’t. One of the main culprits of shoulder pain is a lazy rotator cuff. We don’t see it, so we forget about it. However, this group of muscles is active during function and sport. Whether your playing golf, cleaning the windows or swimming laps in the pool, this cuff is imperative for healthy shoulder movement.
I have told my patients for years that the rotator cuff is “the core of the shoulder”. However, when we hear the term “core” we instantly think of our abdominal muscles (and please add glutes and scapular muscles to that picture). Most of us don’t consider that other areas have a core.
CORE: the central and most important part of something.
What is the Rotator Cuff?
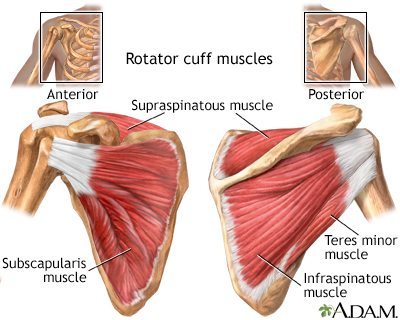 [1]Cuff comes from the latin word cuffia, meaning “head covering”. The rotator cuff is comprised of four muscles: subscapularis, supraspinatus, infraspinatus and teres minor. These muscles attach to the scapula (shoulder blade) and insert onto the humerus (upper arm). In their travel from scapula to humerus, they cover the head of the humerus.
[1]Cuff comes from the latin word cuffia, meaning “head covering”. The rotator cuff is comprised of four muscles: subscapularis, supraspinatus, infraspinatus and teres minor. These muscles attach to the scapula (shoulder blade) and insert onto the humerus (upper arm). In their travel from scapula to humerus, they cover the head of the humerus.
The rotator cuff controls and creates rotation of the arm in the shoulder socket. Simply, the subscapularis rotates the arm in while the infraspinatus and teres minor rotate the arm out. The supraspinatus helps a bit here and there. The cuff doesn’t just move the arm in and out. In fact, it has a very important and interesting role in the shoulder joint.
When we move our arm forward (flexion) or out to the side (abduction) to reach overhead, the rotator cuff is very active before 90º. With these movements, it is not rotating the arm…so what the heck is it doing? It is positioning the humeral head in the perfect spot.
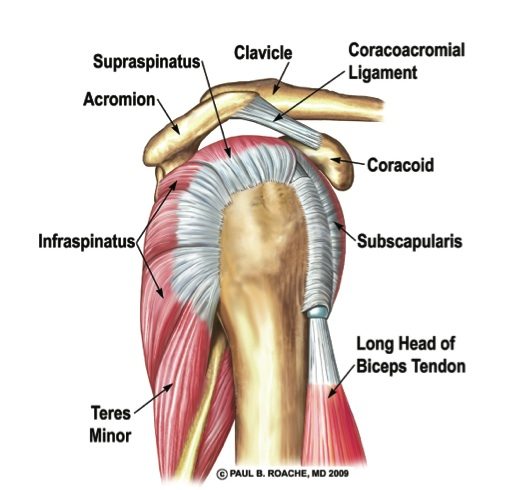 [2]When we move our arm overhead, the rotator cuff is one of the first muscle groups to activate. It is considered the dynamic stabilizer (ahem, core) of the shoulder socket. Initially, the subscapularis and infraspinatus “turn on” to create tension on the humeral head (supraspinatus joins the group around 30º and teres minor assists infraspinatus). This tension “sits” or depresses the humeral head down into the socket. This depressed position keeps the arm from bumping into the acromion (part of the shoulder blade) as the arm moves overhead. This is über important. If the rotator does not perform this portion of the program, pain and dysfunction will develop.
[2]When we move our arm overhead, the rotator cuff is one of the first muscle groups to activate. It is considered the dynamic stabilizer (ahem, core) of the shoulder socket. Initially, the subscapularis and infraspinatus “turn on” to create tension on the humeral head (supraspinatus joins the group around 30º and teres minor assists infraspinatus). This tension “sits” or depresses the humeral head down into the socket. This depressed position keeps the arm from bumping into the acromion (part of the shoulder blade) as the arm moves overhead. This is über important. If the rotator does not perform this portion of the program, pain and dysfunction will develop.
Real World Example: Consider a police officer helping someone into the back of a police car. What is one of the classic motions they always do? They place their hand on the head of the person to depress their head down so it doesn’t hit the top of the car. That’s basically what the rotator cuff is doing every time the shoulder moves overhead.
Blog Activity
Raise your arm out to the side and try to touch your biceps to your ear. Is it pain-free? I hope so. Relax your arm down.
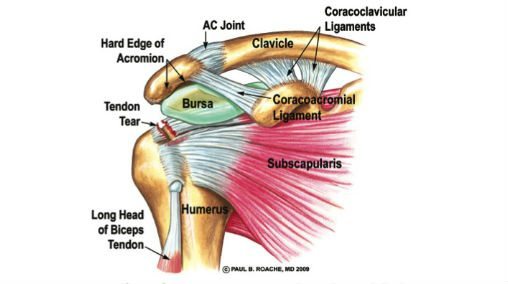 [3]Now, imagine your rotator cuff is injured or torn. Raise your arm to the side and stop at about 60. Because the cuff is injured, the humeral head is not depressed and riding really close to the acromion. If you keep moving the arm up toward your ear, you will feel pain. Why? Because the humeral head begins to “jam” into the acromion and squish the bursa and supraspinatus tendon. Ouchy.
[3]Now, imagine your rotator cuff is injured or torn. Raise your arm to the side and stop at about 60. Because the cuff is injured, the humeral head is not depressed and riding really close to the acromion. If you keep moving the arm up toward your ear, you will feel pain. Why? Because the humeral head begins to “jam” into the acromion and squish the bursa and supraspinatus tendon. Ouchy.
Common Injuries Associated with the Rotator Cuff
- Shoulder impingement: exactly what I just described above. The rotator cuff has been injured (torn or strained) and not working well to depress the humeral head. Thus, it impinges the structures above.
- Rotator Cuff Strain: micro-tearing of one of the four muscles and associated tendon. The strain makes the muscle weak and shoulder impingement results.
- Rotator Cuff Tear (partial): depending on the depth and location of the tear, these will often heal WITHOUT surgery. Good rehab can heal the tear with time.
- Rotator Cuff Tear (complete): usually requires a visit with the orthopedic MD if you’d like to use your shoulder overhead again.
Side note: Shoulder bursitis is a common diagnosis. And, yes, the bursa of the shoulder can become inflamed (called bursitis). Most people will state having an injection to relieve the pain, but did it really solve the problem? Likely not. It’s sad to blame the bursa when it is actually the rotator cuff’s laziness that allowed the bursa to be squished and inflamed. Injections are great for pain relief, but if you want it to go away, fix the issue.
New research
The subscapularis is the anterior (front) muscle of the rotator cuff. It has lower and upper fibers, each having a distinct nerve supply. What this indicates is that upper and lower portion can act independently of each other. And, they do.
With EMG (electromyographic) studies, the lower subscapularis fibers are being praised for their ability to create A LOT of stabilization. The lower fibers are rockstars during overhead movement (flexion and abduction) and moving the arm out (external rotation). The theory is that the lower fibers are more important to counter-balance the tension of the infraspinatus AND resist the shear forces of the deltoid as the arm goes overhead.
In the past, there has been an emphasis on external rotation to activate the rotator cuff. Incorporating the new research, internal rotation may be even more important to stimulate those lower fibers.
Take Home Points
- The rotator cuff stabilizes the humeral head in the shoulder socket for healthy movement = CORE
- Internal rotation may be more beneficial than external rotation when training the rotator cuff
- If you move your arm overhead for any activity (that’s everyone!), the rotator cuff should be trained
 [4]If you enjoyed this post, please share! If you or anyone you know are in need of physical therapy, please contact me [5].
[4]If you enjoyed this post, please share! If you or anyone you know are in need of physical therapy, please contact me [5]. - Subscribe to the blog with your email. You will only receive an email when a new post publishes. Thanks for reading! Lori
References
Heuberer P, Kranzl A, Laky B, Anderl W, Wurnig C. Electromyographic analysis: shoulder muscle activity revisited. Arch Orthop Traum Surg. 2015;135(4):549-63.
Wickham J, Pizzari T, Balster S, Ganderton C, Watson L. The variable roles of the upper and lower subscapularis during shoulder motion. Clin Biomech. 2014;29:885-891.